Have you recently crossed into your 40s? You might notice the scale creeping up. This often happens even if you make zero changes to your diet or exercise routine. If so, you are definitely not alone.
Many women feel frustrated by sudden metabolic shifts during midlife. The frustrating truth is that calorie intake alone does not explain everything happening in your body right now.
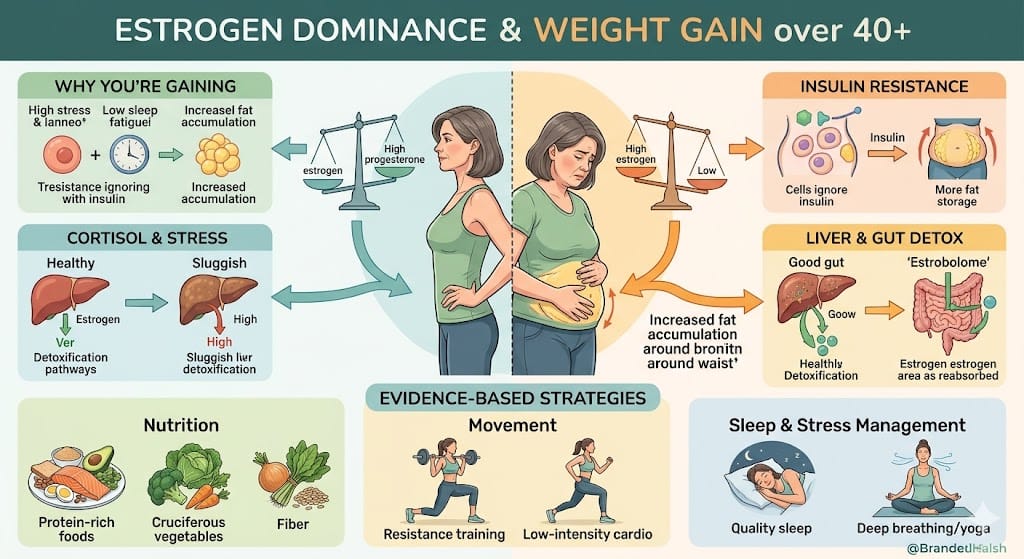
In fact, hormonal shifts fundamentally alter how your body stores fat. Specifically, estrogen dominance perimenopause weight gain changes how you utilize energy and respond to stress.
During your reproductive years, your hormones operated on a predictable monthly rhythm. But as you enter perimenopause, this rhythm becomes highly erratic.
Estrogen levels can fluctuate wildly. Meanwhile, progesterone steadily declines. Consequently, this creates a state of hormonal imbalance that directly impacts your metabolism.
In this comprehensive guide, you will learn the evidence-based science behind midlife body changes. First, we will explore why weight gain becomes so common after 40.
Next, we will discuss how hormonal fluctuations influence body fat distribution. Finally, you will learn actionable, medically sound strategies to reclaim your metabolic health.
What Is Estrogen Dominance?
The term “estrogen dominance” frequently appears in functional medicine. However, it requires careful context to understand properly from a medical perspective. In traditional endocrinology, doctors view hormone imbalances through the lens of absolute excess or deficiency. For instance, they look for extremely high estrogen or menopausal estrogen depletion.
On the other hand, functional medicine looks at the ratios between hormones.
Relative Estrogen Dominance
Estrogen dominance does not always mean your body produces massive, abnormal amounts of estrogen. Instead, it more commonly refers to a progesterone estrogen ratio imbalance.
Progesterone acts as your body’s natural counterweight to estrogen. While estrogen stimulates tissue growth, progesterone stabilizes and calms.
During perimenopause, you stop ovulating consistently. As a result, your progesterone levels drop drastically. Even if your estrogen levels stay within a “normal” range, the lack of progesterone leaves estrogen unchecked. This relative dominance explains why you might experience severe hormone imbalance symptoms women report often. You can feel these symptoms even when a basic blood test shows “normal” estrogen levels.
Understanding this difference is crucial. An absolute high estrogen level happens due to certain ovarian conditions or excess body fat. Conversely, relative estrogen dominance happens due to anovulatory cycles. This missing balance is why your body suddenly resists weight loss.
Why Perimenopause Changes Hormone Balance
Perimenopause is the transitional phase leading up to menopause. It typically begins in a woman’s early to mid-40s. Furthermore, it can last anywhere from four to ten years. The primary hallmark of perimenopause hormone changes is hormonal unpredictability.
Declining Progesterone: Your body forms a corpus luteum only after it releases an egg during ovulation. The corpus luteum produces your progesterone. As ovarian reserve declines, women begin to experience anovulatory cycles. This means they have menstrual cycles without releasing an egg. Consequently, no ovulation means virtually no progesterone production for that month.
Fluctuating Estrogen: Unlike the steady decline of progesterone, estrogen levels resemble a rollercoaster. Your brain pumps out more Follicle-Stimulating Hormone (FSH). It does this to force the aging ovaries to ovulate. As a result, you experience massive, erratic spikes in estrogen, followed by sharp drops.
Ovulatory Changes: The brain-ovary communication axis becomes less efficient. Ultimately, these erratic ovulatory changes cause both heavy periods and metabolic disturbances.
Timeline of Hormonal Changes (Ages 40–55)
| Age Range | Typical Hormonal Shift | Common Physical & Metabolic Impact |
| 35–40 | Subtle progesterone decline. | Slightly shorter menstrual cycles; mild PMS changes. |
| 40–45 | Early perimenopause begins. Anovulatory cycles start. | Unexplained weight gain; heavy bleeding; mood swings. |
| 45–50 | Late perimenopause brings frequent missed periods. | Significant belly fat menopause accumulation; hot flashes. |
| 50–55 | Menopause occurs (12 months without a period). | Loss of protective metabolic effects; muscle loss. |
Estrogen Dominance Perimenopause Weight Gain Explained
Why does a shift in the progesterone to estrogen ratio lead to a larger waistline? The connection between estrogen dominance perimenopause weight gain and your belly comes down to cellular metabolism.
Increased Belly Fat Storage
Estrogen plays a key role in where your body stores fat. During your peak reproductive years, healthy estrogen levels direct fat storage to the hips and thighs. However, estrogen eventually fluctuates and drops. As the progesterone buffer disappears, the body shifts to storing visceral fat. This is the deep abdominal fat that wraps around your organs. Furthermore, this belly fat is metabolically active. It can independently produce its own estrogen, which fuels the imbalance further.
Reduced Metabolic Flexibility
Proper estrogen levels help maintain insulin sensitivity. The unpredictable hormonal landscape of perimenopause often triggers insulin resistance menopause changes. When your cells resist insulin, your pancreas must pump out more of it. High insulin levels signal your body to store fat around the abdomen. Additionally, high insulin blocks the breakdown of stored fat for energy.
Water Retention
Estrogen causes the body to retain sodium and water. In contrast, progesterone acts as a natural diuretic. In a state of relative estrogen dominance, the lack of progesterone allows unchecked water retention. Therefore, you feel constant bloating and see artificial weight gain on the scale.
Increased Appetite and Cravings
Estrogen and progesterone deeply influence hunger hormones like leptin and ghrelin. Erratic estrogen spikes trigger intense cravings for simple carbohydrates. Your brain actively seeks quick energy and dopamine hits to combat perimenopausal fatigue.
Reduced Muscle Mass
As women age, they naturally lose muscle mass. Muscle is highly metabolically active. Because you have less muscle, you develop a lower resting metabolic rate. Consequently, you burn fewer calories simply existing than you did in your 30s.
7 Signs Hormones May Be Contributing to Weight Gain
How do you know if your weight gain is driven by age, diet, or hormones? The following symptoms are strong indicators that your endocrine system is struggling.
Rapid Abdominal Weight Gain: Hormonal weight gain often manifests rapidly. Specifically, it centers almost exclusively around the waistline.
Breast Tenderness: Swollen, sore breasts are a classic sign of high circulating estrogen. This happens when you lack sufficient progesterone to calm the breast tissue.
Heavy or Irregular Periods: Estrogen thickens the uterine lining. Without enough progesterone to stabilize this lining, it sheds heavily and unpredictably.
Mood Swings: Progesterone converts into a neurosteroid that produces a calming effect. Therefore, a lack of progesterone can cause severe anxiety and irritability.
Fatigue: Hormonal chaos taxes the central nervous system. This leads to profound exhaustion that sleep simply cannot fix.
Sleep Disturbances: Waking up at 3:00 AM is incredibly common in perimenopause. This usually occurs due to drops in progesterone and spikes in cortisol.
Brain Fog: Fluctuating estrogen impacts neurotransmitter production. Consequently, you might experience difficulty concentrating and frequent memory lapses, which are common perimenopause brain fog symptoms.
Patient Example: Consider Sarah, 44. She eats a healthy Mediterranean diet and attends spin class weekly. This exact routine kept her fit in her 30s. Yet, she recently gained 12 pounds around her midsection. She is a textbook example of a woman struggling with abdominal fat during perimenopause. Her changing insulin sensitivity and shifting estrogen ratios are driving the weight gain, despite her excellent diet.
The Cortisol–Estrogen Feedback Loop
You cannot discuss reproductive hormones without discussing stress hormones. Indeed, the endocrine system operates as an interconnected web.
The cortisol estrogen feedback loop forms a critical component of midlife weight gain. Cortisol is your body’s primary stress hormone. Your adrenal glands produce it. During perimenopause, ovarian hormone production falters. As a result, the brain relies more heavily on the adrenal glands for hormonal support.
However, many women are chronically stressed. They juggle careers, raise teenagers, and care for aging parents. When this happens, your adrenal glands prioritize cortisol production over other hormones. Elevated cortisol raises blood sugar levels. Next, this blood sugar spike increases insulin, which drives more belly fat storage. Furthermore, high cortisol suppresses the brain’s signaling to the ovaries. This worsens ovulatory dysfunction and ruins the progesterone-to-estrogen ratio.
Sleep disruption plays a massive role here too. Poor sleep increases morning cortisol levels. Consequently, this increases insulin resistance the next day. You must manage this stress-hormone connection through practical stress-management considerations.
Patient Example: Elena, 46, experienced severe fatigue and cycle irregularities. She pushed herself through high-intensity interval training (HIIT) daily to fight her weight gain. Unfortunately, she kept her cortisol chronically elevated. This shut down her natural reproductive rhythms and worsened her estrogen dominance symptoms.
Xenoestrogens Dietary Sources and Environmental Exposure
An important concept in modern hormone imbalance involves endocrine disruptors. These external chemicals mimic estrogen in the body. They bind to estrogen receptors and add to your total estrogenic load.
You cannot completely eliminate exposure in the modern world. However, a balanced, evidence-based discussion acknowledges that heavy exposure to xenoestrogens can worsen relative estrogen dominance.
Common Sources of Endocrine Disruptors:
Plastics: Plastic water bottles and food storage containers contain Bisphenol A (BPA). These are known xenoestrogens.
Personal Care Products: Lotions and cosmetics contain phthalates and parabens. These chemicals easily absorb through the skin.
Food Packaging: PFAS (forever chemicals) can leach into food, particularly when heated.
Dietary Sources: Conventionally raised meats may contain synthetic hormones. Additionally, certain pesticides sprayed on produce have estrogenic properties.
Reducing exposure involves simple steps. First, swap plastic food storage for glass. Second, never microwave food in plastic. Third, choose phthalate-free personal care products. Finally, opt for organic produce where financially feasible.
Liver Estrogen Detoxification Pathway
Estrogen does not just evaporate once it finishes its job. Your body must break it down and eliminate it. If your body cannot process used estrogen efficiently, the hormone recirculates. This worsens the dominance. The liver estrogen detoxification pathway involves two main phases in the liver.
Phase I Detoxification
First, enzymes in the liver metabolize circulating estrogen. They turn the hormone into different metabolites. Some of these metabolites are highly reactive and need immediate neutralization.
Phase II Detoxification
Next, this phase attaches a molecule to the reactive estrogen metabolite. This neutralizes the estrogen and makes it water-soluble. Consequently, your body can excrete it. Nutritional support is essential here. You need sufficient B vitamins, magnesium, and amino acids for Phase II to function optimally.
The Gut-Liver Connection
Finally, the liver sends processed estrogen to the gut for expulsion in your stool. However, poor gut health causes problems. Certain gut bacteria can produce an enzyme called beta-glucuronidase. This enzyme breaks the bond made in Phase II. As a result, your bloodstream reabsorbs the active estrogen.
Evidence-Based Estrogen Detox Support:
Fiber Intake: Consuming 25-35 grams of fiber daily binds to excreted estrogen in the gut. This ensures it leaves the body permanently.
Cruciferous Vegetables: Broccoli and cauliflower contain DIM. This compound strongly supports healthy Phase I estrogen metabolism.
Alcohol Consumption: Alcohol severely taxes the liver. When the liver metabolizes alcohol, it pushes estrogen detoxification aside. Therefore, reducing alcohol quickly improves estrogen metabolism.
Note: Please beware of unsupported “detox” supplements. The liver and gut do the detoxifying naturally. Your job is simply to provide them with the right nutrients.
Testing Hormone Imbalances
When you experience symptoms of hormonal weight gain, testing provides much-needed clarity. However, you must understand the limitations of different testing methods.
Standard Blood Testing
Conventional endocrinology relies on serum (blood) testing. Blood tests provide a helpful snapshot of thyroid function or fasting insulin. However, blood tests have significant limitations during perimenopause. Hormones fluctuate hourly. Therefore, a single blood draw might show “normal” levels if taken on a day when estrogen dips naturally.
Patient Example: Maria, 47, complained of 15 pounds of rapid weight gain and severe mood swings. Her blood work came back “perfectly normal.” Her doctor dismissed her. Unfortunately, standard blood tests did not capture the erratic estrogen spikes occurring later in her cycle.
DUTCH Hormone Test Interpretation
Functional medicine often utilizes the DUTCH test (Dried Urine Test for Comprehensive Hormones). Rather than taking a single snapshot, the DUTCH test looks at hormone metabolites in urine over a 24-hour period.
What it shows: It measures total estrogen and progesterone production. More importantly, it shows how your liver processes estrogen through the detoxification pathways.
Limitations: Traditional medical organizations do not always recognize the DUTCH test as a standard diagnostic tool. Additionally, it can be quite expensive. However, functional medicine practitioners find DUTCH hormone test interpretation highly valuable.
Evidence-Based Strategies to Manage Hormonal Weight Gain
Managing estrogen dominance requires a multi-pronged approach. You must address both the physiological shifts and the metabolic consequences.
Nutrition and Metabolic Health
Protein Intake: To combat muscle loss and stabilize blood sugar, protein is absolutely non-negotiable. Aim for 1.2 to 1.6 grams of protein per kilogram of body weight. Protein triggers satiety hormones, which help manage perimenopausal appetite increases.
Carbohydrate Quality: You do not need to fear carbohydrates. However, you must change the type. Replace simple sugars with complex, high-fiber carbohydrates. This specifically supports your gut microbiome.
Movement and Body Composition
Resistance Training: Lifting weights is the most effective evidence-supported strategy for midlife weight gain. It builds muscle tissue, which directly improves insulin sensitivity.
Zone 2 Cardio: Low-intensity cardio improves mitochondrial health. Importantly, it burns fat without aggressively spiking cortisol levels.
Sleep and Stress Optimization
Sleep: You must treat sleep as a primary medical intervention. Keep your room cool and avoid alcohol before bed. Consistent sleep regulates your circadian rhythm.
Stress Management: Incorporate active relaxation techniques daily. Deep breathing or daily walks in nature signal to your nervous system that you are safe. As a result, your adrenal glands lower cortisol production.
Medical Treatment Options
When lifestyle interventions fall short, you should consider medical treatments.
Menopausal Hormone Therapy (MHT): The North American Menopause Society supports MHT for symptomatic perimenopausal women. For estrogen dominance, a doctor may prescribe bioidentical progesterone. This balances erratic estrogen, protects the uterine lining, and improves sleep.
Insulin Sensitizers: In cases of severe insulin resistance, healthcare providers may discuss specific medications or supplements. These options help restore insulin sensitivity and curb visceral fat.
When to Speak With a Healthcare Professional
Weight gain and mild symptoms are normal parts of the perimenopausal transition. However, certain red flags require prompt medical evaluation. Speak with an Ob/Gyn or certified menopause practitioner if you experience:
Sudden weight gain: Gaining 10 pounds in a single month without lifestyle changes requires investigation.
Abnormal bleeding: Bleeding between periods or extremely heavy periods warrants immediate medical attention.
Severe fatigue: Exhaustion that impedes daily function could indicate thyroid dysfunction.
Significant metabolic changes: A sudden rise in fasting blood glucose or blood pressure requires a doctor’s care.
Frequently Asked Questions
1. Can estrogen dominance perimenopause weight gain be reversed?
Yes. You can reverse it by addressing the root causes. Specifically, improve insulin sensitivity through resistance training and support liver detoxification pathways with fiber. Furthermore, targeted progesterone therapy can help shift your body composition back to a healthier state.
2. Why am I gaining weight in perimenopause when I eat the same?
During perimenopause, declining hormones cause a reduction in muscle mass. This decreases your insulin sensitivity. Therefore, your body requires fewer calories to maintain its weight. The calories you consume are more likely stored as visceral fat.
3. What is the DUTCH hormone test?
The DUTCH test is an advanced functional medicine test. It measures hormone levels and their metabolites over a 24-hour period. Importantly, it provides a detailed look at your progesterone-to-estrogen ratio and cortisol patterns.
4. Can hormone replacement therapy help with weight gain?
Yes, it can. Evidence shows systemic Menopausal Hormone Therapy (MHT) helps prevent the shift of fat storage to the abdomen. By stabilizing hormones, MHT improves sleep and insulin sensitivity. Consequently, this makes it easier to maintain a healthy weight.
5. Is estrogen dominance medically recognized?
Traditional endocrinology uses terms like “anovulatory bleeding” rather than “estrogen dominance.” However, the underlying physiological state is identical. Normal or high estrogen existing without sufficient progesterone is a widely recognized medical phenomenon.
6. How does progesterone affect weight?
Progesterone acts as a natural diuretic. It helps reduce water retention and bloating. Furthermore, it supports thyroid function and improves sleep quality. Better sleep naturally leads to improved insulin sensitivity.
7. Does belly fat produce its own estrogen?
Yes, it does. Adipose tissue contains an enzyme called aromatase. This enzyme converts circulating androgens into estrogen. Therefore, this creates a vicious cycle where belly fat produces even more estrogen.
8. What are xenoestrogens and how do they impact me?
Xenoestrogens are synthetic chemicals found in plastics and personal care products. They mimic estrogen in the body. Consequently, they bind to your estrogen receptors and amplify hormone imbalance symptoms.
9. How can I support my liver estrogen detoxification pathway?
First, reduce your alcohol consumption. Second, eat a diet rich in cruciferous vegetables like broccoli. Third, consume adequate protein and ensure daily bowel movements through high fiber intake.
10. Does high cortisol cause estrogen dominance?
Yes, chronic stress keeps cortisol levels elevated. High cortisol suppresses the brain-ovary communication axis. This leads to absent ovulation. Without ovulation, you lack progesterone, which directly results in relative estrogen dominance.
Conclusion
Navigating the midlife transition often feels like an uphill battle. This is especially true when you face estrogen dominance perimenopause weight gain despite your best efforts. Understanding this physiological shift is the first crucial step toward reclaiming your health.
The hormonal shifts after 40 create a perfect storm for metabolic changes. Erratic estrogen spikes, declining progesterone, and insulin resistance all drive visceral fat accumulation. The weight gain mechanisms you experience are deeply rooted in cellular biology.
While traditional medicine sometimes overlooks these nuances, recognizing the signs empowers you to take action. You can implement practical lifestyle strategies today.
Prioritize a high-protein diet and engage in resistance training. Furthermore, support your liver’s detoxification pathways and manage your stress levels daily.
Remember, you do not have to suffer in silence. The importance of medical evaluation cannot be overstated. Work with a healthcare professional who truly understands midlife women’s health.
By addressing the root hormonal cause, you can stop midlife weight gain entirely. Ultimately, you can step into your next chapter with renewed energy and confidence.