Discovering a genetic mutation in your family line often brings immediate questions and understandable anxiety. Unlocking the complexities of your genetic profile empowers you to make highly informed healthcare decisions. Specifically, understanding the BRCA1 vs BRCA2 mutation cancer risk differences remains essential for anyone navigating hereditary cancer syndromes.
Both BRCA1 and BRCA2 genes play critical roles in protecting your body from cancer. However, mutations in these genes do not behave identically.
They carry distinct lifetime risks, affect different organs, and influence the age when cancer might develop. Consequently, interpreting these unique risk profiles is absolutely critical for effective clinical management.
In this guide, you will learn exactly how these two genetic mutations differ. We will explore cancer risk variations, age of onset differences, and evidence-based screening strategies. Furthermore, we will review preventive treatment options and clinical decision pathways grounded in the latest oncology research.
What Are BRCA Genes?
To understand hereditary cancer risks, you must first understand how healthy genes function. BRCA stands for “BReast CAncer gene.” Every human inherits two copies of the BRCA1 and BRCA2 genes, one from each parent.
Importantly, these are tumor suppressor genes. Their primary job involves preventing cells from growing and dividing too rapidly. Specifically, they produce proteins that help repair damaged DNA through a process called homologous recombination. When DNA breaks occur, BRCA proteins step in to fix the damage, maintaining the genetic stability of your cells.
What happens when a mutation occurs? If you inherit an altered, or mutated, BRCA gene, your body loses a crucial layer of cellular defense. The damaged DNA cannot repair itself efficiently. Consequently, cells can begin to grow uncontrollably, leading to cancer development.
These genetic mutations follow an autosomal dominant inheritance pattern. Therefore, if one parent carries a BRCA mutation, you have a 50% chance of inheriting that exact mutation.
BRCA1 vs BRCA2 Mutation Cancer Risk Differences
While both mutations significantly elevate cancer risk, their clinical profiles differ substantially. The BRCA1 vs BRCA2 mutation cancer risk differences directly dictate how oncologists design your screening and prevention protocols.
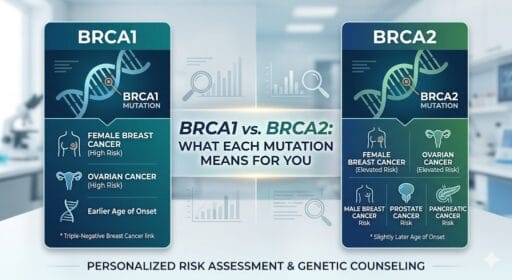
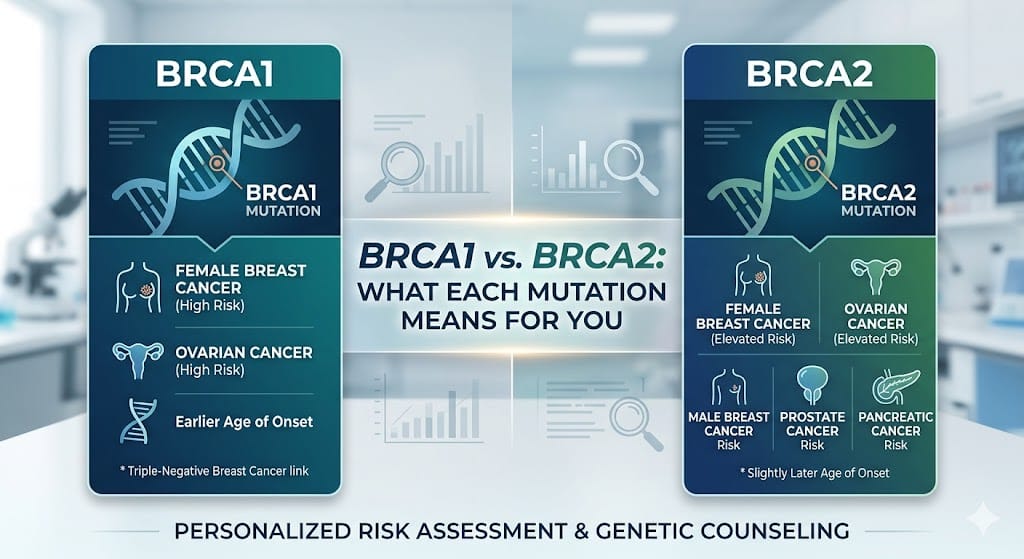
Firstly, the specific cancer types vary between the two genes. BRCA1 mutations strongly associate with female breast and ovarian cancers. Conversely, BRCA2 mutations trigger a broader spectrum of disease. BRCA2 increases the risk for female breast and ovarian cancer, but it also significantly elevates the risk for prostate cancer, pancreatic cancer, and male breast cancer.
Secondly, the age of onset differs notably. BRCA1-related cancers typically develop at a younger age. Women with BRCA1 mutations often face breast cancer diagnoses in their 30s or 40s.
Meanwhile, BRCA2-related cancers tend to occur slightly later in life, often mirroring closer to average age ranges, though still earlier than the general population.
Finally, the aggressiveness of the resulting cancers varies. BRCA1 mutations frequently lead to more aggressive, fast-growing tumors. In contrast, BRCA2 mutations often result in tumors that grow slightly slower, though they remain highly dangerous without proactive intervention.
Side-by-Side Cancer Risk Comparison (NCCN 2025 Data)
Understanding your specific statistical risk requires up-to-date clinical data. The following table highlights the estimated lifetime risks associated with each mutation, based on the NCCN 2025 Genetic/Familial High-Risk Assessment Guidelines.
| Cancer Type | BRCA1 Lifetime Risk | BRCA2 Lifetime Risk | General Population Risk |
| Breast cancer (female) | 65% – 72% | 45% – 69% | ~13% |
| Ovarian cancer | 39% – 44% | 11% – 17% | ~1.2% |
| Pancreatic cancer | 1% – 5% | 5% – 10% | ~1.5% |
| Prostate cancer | ~8.6% | 20% – 60% | ~12.5% |
| Male breast cancer | ~1.2% | 7% – 8% | ~0.1% |
Note: Risk ranges can vary slightly based on family history and specific mutation locations within the gene.
BRCA1 vs BRCA2: Key Clinical Differences
Beyond lifetime percentages, the actual tumor biology differs dramatically between BRCA1 and BRCA2 mutations. This tumor biology directly impacts treatment options and survival outcomes.
BRCA1 mutations strongly link to triple-negative breast cancer (TNBC). Triple-negative tumors lack estrogen receptors, progesterone receptors, and HER2 proteins. Consequently, these tumors do not respond to hormonal therapies. They generally behave more aggressively and require intensive chemotherapy protocols.
In contrast, BRCA2 mutations typically result in hormone receptor-positive (HR+) breast cancers. These tumors rely on hormones like estrogen to grow. Therefore, oncologists can effectively treat BRCA2-related breast cancers with targeted endocrine therapies, such as tamoxifen or aromatase inhibitors.
Furthermore, earlier versus later onset remains a defining clinical difference. A woman discovering a BRCA1 mutation must often initiate high-intensity screening in her mid-20s.
Alternatively, a BRCA2-positive individual might adjust their screening timeline slightly, particularly concerning prostate and pancreatic surveillance, which typically begins later.
Hereditary Breast Ovarian Cancer Syndrome (HBOC)
Medical professionals classify BRCA mutations under the umbrella of hereditary breast ovarian cancer syndrome (HBOC). HBOC signifies an inherited predisposition to specific malignancies, driven primarily by BRCA1 and BRCA2 mutations.
Understanding what HBOC means helps families track disease patterns across generations. Not everyone needs genetic testing. However, oncologists strongly recommend testing for individuals meeting specific family history criteria.
Who should get tested? You should consider testing if you observe specific red flags in your family history.
These red flags include multiple relatives with breast cancer, breast cancer diagnosed before age 50, or any family member with ovarian cancer. Furthermore, male breast cancer, pancreatic cancer, or metastatic prostate cancer in your family tree strongly warrants genetic evaluation.
Because HBOC follows an autosomal dominant inheritance pattern, the risk does not skip generations. If a parent carries the gene, each child faces a 50% inheritance risk, regardless of gender.
Genetic Counselling for BRCA Positive Patients
Navigating a genetic diagnosis requires professional guidance. Therefore, genetic counselling BRCA positive protocols are essential for interpreting your risk accurately and planning your next steps.
Genetic counselors serve as specialized healthcare providers. They translate complex genetic data into actionable medical strategies.
During a session, a counselor will map out your family pedigree, calculate your personalized risk percentages, and explain the clinical implications of your specific mutation.
Consider Sarah, a 35-year-old woman discovering a BRCA1 mutation after a family history of early-onset breast cancer. Her genetic counselor helped her interpret the immediate risks, leading to a coordinated plan involving early MRI surveillance.
Furthermore, genetic counselors facilitate family cascade testing. If you test positive, your blood relatives must be informed so they can pursue their own testing. This process often brings significant emotional and ethical considerations.
A skilled counselor helps you navigate these difficult family conversations, ensuring your relatives receive accurate information without unnecessary panic.
Prophylactic Mastectomy BRCA Criteria
For many high-risk patients, surgical prevention offers the most effective peace of mind. Understanding the prophylactic mastectomy BRCA criteria helps you make informed choices about risk-reducing surgeries.
Prophylactic, or risk-reducing, mastectomy involves surgically removing the breast tissue before cancer develops. Who qualifies for this procedure? Generally, any individual carrying a pathogenic BRCA1 or BRCA2 mutation qualifies for prophylactic surgery under NCCN guidelines.
Take Elena, a patient considering preventive surgery after genetic counseling. She navigated the prophylactic mastectomy BRCA criteria with her care team to balance profound risk reduction with her quality of life.
The risk-reduction benefits are staggering. A bilateral prophylactic mastectomy can reduce breast cancer risk by 90% to 95% in BRCA-positive women.
Timing considerations remain deeply personal. Many women schedule this surgery between ages 25 and 40, depending on their family history and family planning goals. However, surgery is not mandatory. Alternative surveillance options exist for women who decline or delay surgery, involving intensive, alternating imaging schedules.
Screening and Surveillance Guidelines
If you choose to delay or decline preventive surgery, you must adhere to strict screening and surveillance guidelines. Early detection remains your best defense against hereditary cancers.
For breast cancer, high-risk screening typically begins at age 25. Women undergo an annual breast MRI with contrast. By age 30, guidelines recommend alternating the MRI with an annual 3D mammogram every six months. This aggressive schedule catches tumors when they are small and highly treatable.
Unfortunately, ovarian cancer screening limitations pose a significant challenge. Currently, transvaginal ultrasounds and CA-125 blood tests do not reliably detect ovarian cancer in its early stages.
Therefore, oncologists strongly recommend risk-reducing salpingo-oophorectomy (removal of ovaries and fallopian tubes) between ages 35 and 45.
For men, surveillance focuses heavily on prostate and breast tissue. Conversely, look at David, a BRCA2-positive individual concerned about male breast or prostate cancer. His clinical timeline prioritizes baseline PSA screening starting at age 40, followed by annual clinical breast exams.
Finally, pancreatic cancer surveillance in high-risk cases is evolving. NCCN guidelines now recommend annual endoscopic ultrasounds or specialized MRIs for BRCA carriers who also have a first- or second-degree relative with pancreatic cancer, starting at age 50.
Treatment Advances: Olaparib and PARP Inhibitors
Historically, BRCA-related cancers received standard chemotherapy protocols. Today, precision oncology has revolutionized treatment. Specifically, the introduction of the olaparib PARP inhibitor BRCA pathway offers targeted, highly effective therapy.
How do PARP inhibitors work? PARP is an enzyme that helps repair single-strand DNA breaks. If you block PARP in a normal cell, the cell can still repair its DNA using the BRCA pathway. However, BRCA-mutated cancer cells already have broken BRCA pathways.
Therefore, when a PARP inhibitor blocks their only remaining repair mechanism, the cancer cells accumulate too much DNA damage and die. This mechanism of action is called synthetic lethality.
Why do BRCA tumors respond so well? Because their fundamental weakness the inability to repair homologous recombination is directly exploited by the drug.
Olaparib, alongside other PARP inhibitors, plays a massive role in treating advanced breast, ovarian, prostate, and pancreatic cancers. This precision oncology approach significantly extends progression-free survival for BRCA-positive patients.
PALB2 and Other Related Gene Mutations
While BRCA genes dominate the conversation, oncology researchers now recognize several other hereditary cancer risk genes. Specifically, the PALB2 gene mutation has emerged as a major clinical player.
Why does PALB2 matter? PALB2 stands for “Partner and Localizer of BRCA2.” The PALB2 protein physically interacts with the BRCA2 protein to repair DNA.
Consequently, a mutation in PALB2 disrupts this gene interaction network, leading to cancer risks that closely mirror BRCA mutations. PALB2 carriers face significantly elevated risks for breast and pancreatic cancers.
Because of these discoveries, oncologists no longer test for BRCA genes in isolation. Expanded hereditary cancer panels now sequence dozens of genes simultaneously. This comprehensive approach ensures that patients with mutations in PALB2, CHEK2, ATM, or TP53 receive the appropriate surveillance and preventive care.
Emotional and Psychological Impact of BRCA Diagnosis
Receiving a positive BRCA result triggers a complex wave of emotions. Medical guidelines often focus entirely on the physical body, yet the emotional and psychological impact requires equal attention.
Anxiety and uncertainty frequently dominate the initial weeks following a diagnosis. Patients often experience “previvor” syndrome, feeling the heavy burden of cancer risk without an actual cancer diagnosis.
Furthermore, family communication challenges complicate the emotional landscape. Sharing genetic information with parents, siblings, and adult children can induce guilt and defensiveness.
Decision-making stress also takes a heavy toll. Choosing between intensive screening and irreversible prophylactic surgeries requires immense mental resilience. Therefore, the importance of counseling support cannot be overstated.
Engaging with oncology social workers, specialized therapists, and peer support groups is a vital component of holistic genetic care.
Frequently Asked Questions:
1. Is BRCA1 or BRCA2 more dangerous?
Neither gene is inherently more “dangerous,” but they behave differently. BRCA1 typically carries a higher lifetime risk for ovarian cancer and often results in more aggressive, triple-negative breast cancers at a younger age. BRCA2 carries a slightly lower ovarian cancer risk but significantly elevates the risk for male breast, prostate, and pancreatic cancers.
2. What cancers does BRCA2 cause?
A BRCA2 mutation significantly increases the risk of developing female breast cancer, ovarian cancer, male breast cancer, aggressive prostate cancer, and pancreatic cancer. Furthermore, it slightly elevates the risk for melanoma.
3. Should I remove my breasts if I am BRCA positive?
Prophylactic mastectomy reduces your breast cancer risk by up to 95%. However, the decision is deeply personal. Many women opt for high-intensity surveillance (alternating MRI and mammograms) instead of surgery. You must discuss your specific risks with a genetic counselor and oncologist.
4. Can BRCA mutations skip generations?
No, BRCA mutations cannot skip generations. They follow an autosomal dominant inheritance pattern. However, a mutation can appear to skip a generation if a male carrier never develops prostate or male breast cancer, but subsequently passes the gene to his daughter.
5. Does BRCA always cause cancer?
No, carrying a BRCA mutation does not guarantee you will develop cancer. It simply signifies a highly elevated susceptibility. Many individuals with BRCA mutations live long, healthy lives, especially if they strictly adhere to preventive medical guidelines.
6. What is PALB2 gene risk?
PALB2 is a tumor suppressor gene that works alongside BRCA2. Mutations in PALB2 significantly elevate the lifetime risk of female breast cancer, often approaching the risk levels seen in BRCA2 carriers. It also elevates pancreatic cancer risk.
7. How accurate is genetic testing for BRCA?
Clinical genetic testing via blood or saliva in certified diagnostic laboratories is extremely accurate, nearing 99% precision. However, direct-to-consumer DNA kits often miss thousands of clinically significant BRCA variants and should not be used for medical decision-making.
8. Can lifestyle reduce BRCA cancer risk?
While genetics drive the primary risk, healthy lifestyle choices provide secondary protection. Maintaining a healthy BMI, limiting alcohol consumption, exercising regularly, and avoiding smoking can lower overall inflammation and slightly mitigate baseline cancer risks.
9. Are PARP inhibitors only for BRCA mutations?
Initially, yes. However, PARP inhibitors are now approved for cancers demonstrating Homologous Recombination Deficiency (HRD), even if a specific BRCA mutation is not present. They are heavily utilized in ovarian and metastatic breast cancers.
10. When should I start BRCA screening?
If you know you carry a mutation, NCCN guidelines generally recommend starting clinical breast exams at age 25, alongside annual breast MRIs.
Ovarian cancer discussions usually begin around age 35. Men should begin prostate screening discussions by age 40.
Conclusion:
Understanding the distinct BRCA1 vs BRCA2 mutation cancer risk differences fundamentally shifts how you manage your hereditary health. While both genes act as vital tumor suppressors, their mutated forms dictate vastly different clinical pathways.
BRCA1 primarily drives early-onset, aggressive breast and ovarian cancers. Meanwhile, BRCA2 presents a broader threat profile, heavily implicating prostate, pancreatic, and male breast tissues.
Personalized risk interpretation serves as the cornerstone of effective preventive medicine. You cannot rely on generalized statistics to map out your life.
Instead, you must lean into the expertise of certified genetic counselors. These professionals integrate NCCN 2025 guidelines with your unique family history to construct a highly personalized medical blueprint.
Furthermore, you hold immense power over your clinical outcomes. Whether you choose the profound risk reduction of prophylactic surgeries or the vigilant protection of high-intensity MRI surveillance, modern medicine offers robust pathways to keep you safe.
Additionally, breakthroughs in targeted therapies, specifically PARP inhibitors, have transformed the treatment landscape for those who do develop disease.
Ultimately, a genetic diagnosis brings undeniable emotional weight. Acknowledge the anxiety, communicate openly with your family, and utilize professional support systems. By combining clinical vigilance with emotional resilience, you can successfully navigate hereditary cancer risk and prioritize your long-term longevity.