Imagine going to the pharmacy to pick up your new heart failure medication. Suddenly, you notice the label says the drug is for type 2 diabetes. If your blood sugar is completely normal, you might feel confused or even worried. However, you are not alone in this experience.
In a brilliant breakthrough for modern medicine, cardiologists now routinely prescribe sodium-glucose cotransporter 2 (SGLT2) inhibitors to heart failure patients. Crucially, they do this whether the patient has diabetes or not.
Why did this clinical shift happen? It happened because drugs like empagliflozin and dapagliflozin do far more than manage blood sugar. Consequently, these medications radically reduce hospital admissions, protect kidney function, and extend human life. Today, they represent a mandatory foundation of modern heart care.
In this comprehensive guide, you will learn exactly why these former diabetes drugs are now premier heart failure treatments. We will explore how they protect your body, review the massive clinical trials, and explain what the latest medical guidelines mean for you.
Disclaimer: This article is for educational purposes only and should not replace professional medical advice. Always consult your healthcare provider before starting, stopping, or modifying any medication regimen.
What Are SGLT2 Inhibitors?
To understand their power, we must look at how these drugs interact with your body. Originally, pharmaceutical companies designed SGLT2 inhibitors solely to lower blood glucose in adults with type 2 diabetes.
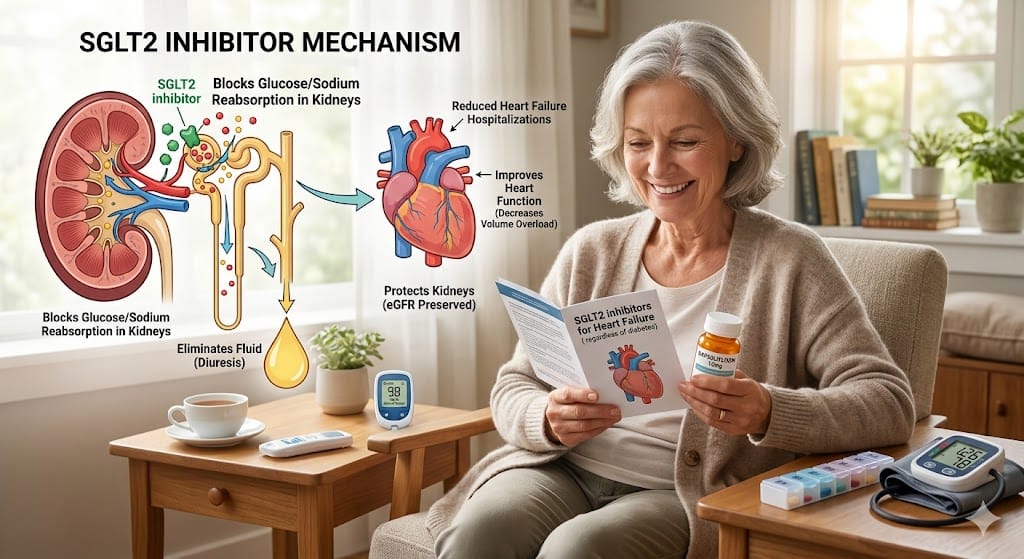
The actual SGLT2 protein resides inside the microscopic filtering tubes of your kidneys. Normally, this protein acts like a sponge. It grabs filtered sugar and sodium from your urine and pulls them back into your bloodstream.
SGLT2 inhibitors completely block this sponge-like action. Therefore, your kidneys stop reabsorbing the excess sugar. Instead, your body flushes the extra glucose out through your urine, which naturally lowers your blood sugar levels.
Major Drugs in This Class
Doctors currently prescribe a few primary medications within this specific drug class:
Empagliflozin: A leading medication heavily proven to provide massive cardiovascular benefits.
Dapagliflozin: A foundational drug widely utilized to treat advanced heart failure.
Canagliflozin: A medication used primarily for diabetic kidney disease.
Ertugliflozin: A drug focused mostly on standard blood sugar control.
Why SGLT2 Inhibitors Work for Heart Failure
When researchers first tested these drugs for safety, they uncovered an unexpected medical miracle. Patients with heart issues were suddenly experiencing fewer emergencies. Soon, cardiologists realized that the benefits extend far beyond metabolic control.
Reduced Cardiac Workload
Because these medications flush out sodium and water, they naturally reduce the total volume of fluid in your blood vessels. Less fluid means lower pressure inside your arteries. Consequently, your heart does not have to pump nearly as hard to move blood through your body.
Natriuresis and Diuresis
Natriuresis means removing sodium through urine, while diuresis means increasing overall urine output. SGLT2 inhibitors act as very gentle, steady diuretics. Unlike traditional fluid pills, they do not cause dangerous drops in potassium or other vital electrolytes. This gentle fluid removal quickly relieves shortness of breath and ankle swelling.
Kidney Protection and Cardiorenal Syndrome
The heart and kidneys work as a tight team. When the heart weakens, it cannot pump enough blood to the kidneys. The kidneys then panic and retain excess salt, which overload the weak heart. This dangerous cycle is called cardiorenal syndrome.
Fortunately, SGLT2 inhibitors break this loop entirely. They lower the physical pressure inside the kidney filters. As a result, they shield long-term kidney function while easing the heart’s workload.
Reduced Cardiac Remodeling
Chronic heart failure forces the heart muscle to stretch, thicken, and scar. Doctors call this structural damage cardiac remodeling. SGLT2 inhibitors slow down or reverse this process because they help the heart burn energy more efficiently. This metabolic shift reduces harmful scarring in the cardiac tissue.
SGLT2 Inhibitors Heart Failure Non-Diabetic Patients: What Changed?
For decades, standard heart failure therapy relied strictly on beta-blockers and blood pressure medications. When SGLT2 inhibitors first arrived, they belonged strictly to diabetes doctors.
However, the medical paradigm shifted rapidly. Researchers suspected that these drugs protected the heart through pathways that had nothing to do with blood sugar. Therefore, they launched bold new clinical trials focusing entirely on heart failure patients who did not have diabetes.
The results completely stunned the medical community. The data proved that SGLT2 inhibitors protect non-diabetic hearts with the exact same efficiency. Today, if a cardiologist explains this therapy, they will describe these drugs as cellular bodyguards rather than simple diabetes pills.
DAPA-HF Trial: The Study That Changed Heart Failure Treatment
The DAPA-HF clinical trial completely revolutionized modern cardiology. It provided the definitive proof that these medications belong in standard cardiovascular care.
Study Design and Patient Population
The trial evaluated over 4,700 patients suffering from heart failure with reduced ejection fraction (HFrEF). Crucially, 55% of these participants did not have diabetes. Researchers split the patients into two groups. One group received 10 mg of dapagliflozin daily, while the other group received a dummy pill.
Key Findings
The final data were absolutely undeniable. Dapagliflozin drastically lowered the risk of cardiac death and emergency hospital visits.
Heart Failure Hospitalisation Reduction: Patients on the medication experienced a massive drop in emergency admissions.
Cardiovascular Death: The drug directly lowered the risk of dying from heart failure complications.
Benefits Without Diabetes: Most importantly, the drug worked perfectly for patients without type 2 diabetes.
Impact on Clinical Practice
Because of this trial, the FDA officially approved dapagliflozin as a primary heart failure treatment, completely independent of a patient’s blood sugar status.
DAPA-HF Trial Summary
| Feature | Trial Details |
| Drug Investigated | Dapagliflozin |
| Target Condition | HFrEF |
| Diabetes Status | Both Diabetic and Non-Diabetic |
| Major Finding | 26% reduction in CV death or worsening heart failure |
EMPEROR-Reduced Trial Results Explained
Right after the DAPA-HF trial, scientists launched the EMPEROR-Reduced trial to test the second major drug in this class: empagliflozin.
Study Design and Outcomes
This major trial tracked over 3,700 patients with HFrEF. Once again, a huge portion of the study group did not have any history of diabetes. Patients took either 10 mg of empagliflozin or a placebo daily.
The trial completely confirmed the previous breakthroughs. Empagliflozin achieved a massive reduction in the combined risk of cardiovascular death and heart failure hospitalizations.
Hospitalisation Reduction and Kidney Protection
The reduction in hospital visits was highly significant. Furthermore, this trial highlighted incredible benefits for renal health. Empagliflozin dramatically slowed down the progressive decline of kidney function, which frequently cripples heart failure patients over time.
EMPEROR-Reduced Trial Summary
| Feature | Trial Details |
| Drug Investigated | Empagliflozin |
| Target Condition | HFrEF |
| Diabetes Status | Both Diabetic and Non-Diabetic |
| Major Finding | 25% risk reduction in HF hospitalization or CV death |
DAPA-HF vs EMPEROR-Reduced Trial Comparison
While both studies proved the class-wide benefits of these drugs, comparing them side-by-side reveals their unique clinical strengths.
| Feature | DAPA-HF | EMPEROR-Reduced |
| Drug | Dapagliflozin | Empagliflozin |
| Patient Count | ~4,744 patients | ~3,730 patients |
| Diabetes Requirement | Not required | Not required |
| Primary Outcome | CV death or worsening HF | CV death or worsening HF |
| Hospitalisation Reduction | Highly significant | Highly significant |
| Mortality Benefit | Clear reduction in CV death | Positive trend toward benefit |
| Kidney Outcomes | Excellent secondary benefits | Strong, proven renal slowing |
| Clinical Significance | First to prove non-diabetic use | Confirmed renal safety shield |
FDA-Approved vs Off-Label Uses
The regulatory landscape changes quickly as new clinical data emerges. This clear table separates officially approved indications from off-label medical practices.
| Drug | FDA Approved Heart Failure Use | Diabetes Use | Off-Label Uses |
| Dapagliflozin | Approved for HFrEF and broader heart failure | Approved for Type 2 Diabetes | Specific cardiorenal syndromic conditions |
| Empagliflozin | Approved for HFrEF and HFpEF types | Approved for Type 2 Diabetes | Acute care immediately after heart attacks |
Note: Doctors do not prescribe SGLT2 inhibitors for type 1 diabetes due to a higher risk of dangerous acid buildup.
Dosing and Eligibility Guide (Cardiologist-Reviewed Style)
Starting an SGLT2 inhibitor is remarkably simple. Unlike older cardiac drugs, these modern medications do not require weeks of slow dosage adjustments.
| Medication | Standard Dose | Renal Function Considerations | Heart Failure Eligibility | Monitoring Requirements |
| Empagliflozin | 10 mg once daily | Avoid if eGFR is extremely low | HFrEF and HFpEF patients | Check blood pressure and kidneys |
| Dapagliflozin | 10 mg once daily | Avoid if eGFR is extremely low | Broadly applicable for HF | Check fluid levels and kidneys |
Clinical Note: Your physician will run a simple blood test to check your estimated glomerular filtration rate (eGFR) before your first dose. This ensures your kidneys have enough filtering power to initiate the therapy safely.
Benefits Beyond Blood Sugar
The phrase “beyond blood sugar” perfectly captures this therapeutic revolution. When you take these pills, multiple systems in your body experience a defensive boost.
Reduced Hospitalisation Risk
Frequent heart failure flare-ups are emotionally exhausting and physically dangerous. Fortunately, SGLT2 inhibitors keep excess fluid off your lungs. This prevents the sudden fluid overloads that force patients into emergency rooms.
Improved Quality of Life
By gently removing extra fluid, these drugs quickly improve your daily life. Your breathing becomes easier, your energy levels rise, and your swollen ankles shrink. Consequently, you can walk further and manage daily chores with far less fatigue.
Kidney Protection and Cardiorenal Benefits
Kidney failure accelerates heart disease, and heart failure rapidly destroys the kidneys. SGLT2 inhibitors actively shield your renal tissue. They reduce dangerous internal pressure in your kidneys, stop protein leakage, and preserve your filtering capacity for years.
Long-Term Cardiovascular Outcomes
Ultimately, the most important benefit is survival. SGLT2 inhibitors keep the heart’s electrical rhythms stable. This directly lowers the risk of sudden cardiac death, giving you more high-quality years with your family.
Potential Risks and Side Effects
Like any effective medication, SGLT2 inhibitors carry certain risks. However, their safety profile is exceptionally clean compared to their life-saving benefits.
Common Side Effects
Because these drugs push sugar out through your urinary system, side effects usually manifest locally.
Genital Infections: Yeast infections are the most common complaint. However, they are easily treated with standard antifungal creams. Maintaining excellent personal hygiene lowers this risk significantly.
Increased Urination: You will likely notice an increase in trips to the bathroom during the first two weeks of treatment.
Serious Side Effects
Volume Depletion and Hypotension: Flushing too much fluid can lead to dehydration and low blood pressure. If you feel dizzy when standing up, your doctor may simply lower your other blood pressure pills.
Ketoacidosis (Rare): This is an extremely rare but serious condition where the blood becomes dangerously acidic. It occurs almost exclusively in patients who have diabetes.
When Patients Should Contact Their Doctor
Contact your clinic immediately if you experience severe dizziness, fainting, intense abdominal pain, constant nausea, or severe pain and swelling in the groin area.
Who Is a Candidate for SGLT2 Inhibitor Therapy?
Today, almost every single patient diagnosed with chronic heart failure is an excellent candidate for this treatment.
HFrEF: Patients with an ejection fraction of 40% or lower receive the strongest recommendation.
HFmrEF: Patients with a mildly reduced ejection fraction (41% to 49%) see great benefits.
HFpEF: Patients with preserved ejection fraction (50% or higher) now have guideline support to take these drugs, marking a massive historical breakthrough.
Non-Diabetic Populations: Individuals without any history of diabetes are equally eligible and receive identical heart protection.
2025 Heart Failure Guideline Recommendations
Major global medical societies have fully updated their protocols. The American College of Cardiology (ACC) and American Heart Association (AHA) place SGLT2 inhibitors at the absolute center of modern care.
Position Within Guideline-Directed Medical Therapy (GDMT)
The medical guidelines award SGLT2 inhibitors a Class 1 recommendation. This is the highest possible medical endorsement. They now officially form one of the four mandatory pillars of heart failure care.
Current Role Alongside Other Therapies
Cardiologists no longer wait months to start these medications. Instead, they introduce them immediately alongside the other three vital lifelines:
Beta Blockers: Medications that protect your heart from dangerous, rapid rhythms.
ARNI Therapy: Advanced blood pressure drugs that relax your blood vessels.
MRAs: Mineralocorticoid receptor antagonists that stop harmful cardiac tissue scarring.
Using all four pillars simultaneously creates a powerful shield that maximizes your lifespan.
Frequently Asked Questions
Can non-diabetic patients take SGLT2 inhibitors?
Yes. These medications are fully approved and highly recommended for heart failure patients who do not have diabetes.
Why are diabetes drugs used for heart failure?
They flush out extra water and sodium. This action rapidly lowers the physical workload on the heart and protects your kidneys.
Which is better, empagliflozin or dapagliflozin?
Both offer exceptional, world-class protection. Your cardiologist will select one based on your insurance coverage and specific kidney scores.
Do SGLT2 inhibitors improve survival?
Yes. Multiple landmark clinical trials prove that these drugs significantly reduce the risk of cardiovascular death.
Are SGLT2 inhibitors safe for kidney disease?
Yes. They are actually highly protective. They slow down the long-term progression of chronic kidney disease.
What are the latest heart failure guidelines?
The current guidelines mandate a four-pillar framework: beta-blockers, ARNIs, MRAs, and SGLT2 inhibitors.
Will SGLT2 inhibitors make my blood sugar drop too low?
No. If you do not have diabetes, your blood sugar will remain perfectly safe and stable.
Do SGLT2 inhibitors replace my water pill?
Not always. You may still need your standard loop diuretic like furosemide, but your doctor might lower the dose.
How quickly do SGLT2 inhibitors work for heart failure?
The clinical benefits begin remarkably fast. Studies show a significant drop in hospitalization risks within the first 30 days.
What is the most common side effect?
The most frequent side effects are mild, easily treatable genital yeast infections caused by sugar in the urine.
Conclusion
The evolution of SGLT2 inhibitors from simple diabetes pills into life-saving heart failure treatments is a monumental victory for modern medicine. Whether you are managing HFrEF, dealing with HFpEF, or protecting yourself from cardiorenal syndrome, medications like empagliflozin and dapagliflozin offer immense hope. They keep you out of the hospital, shield your kidneys, and give you more years to enjoy your life.
Most importantly, the medical science is perfectly clear. You do not need to have diabetes to experience these incredible cardiovascular rewards. The deep data from the DAPA-HF and EMPEROR-Reduced trials prove that these drugs optimize your heart through pathways that are completely separate from blood sugar regulation.
Because every heart is unique, an individualized treatment plan is absolutely vital. Talk to your cardiologist about your guideline-directed medical therapy today. Ensure your care team evaluates you for an SGLT2 inhibitor. Heart failure care has changed completely for the better, and these modern treatments are ready to help you thrive.