Middle-aged women often face a deeply frustrating medical journey. They experience severe exhaustion and breathlessness daily. Yet, their standard cardiac tests look completely perfect. Unfortunately, HFpEF symptoms in women misdiagnosed as anxiety, aging, or simple deconditioning represent a growing cardiology crisis.
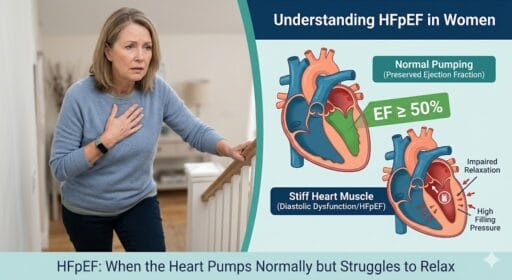
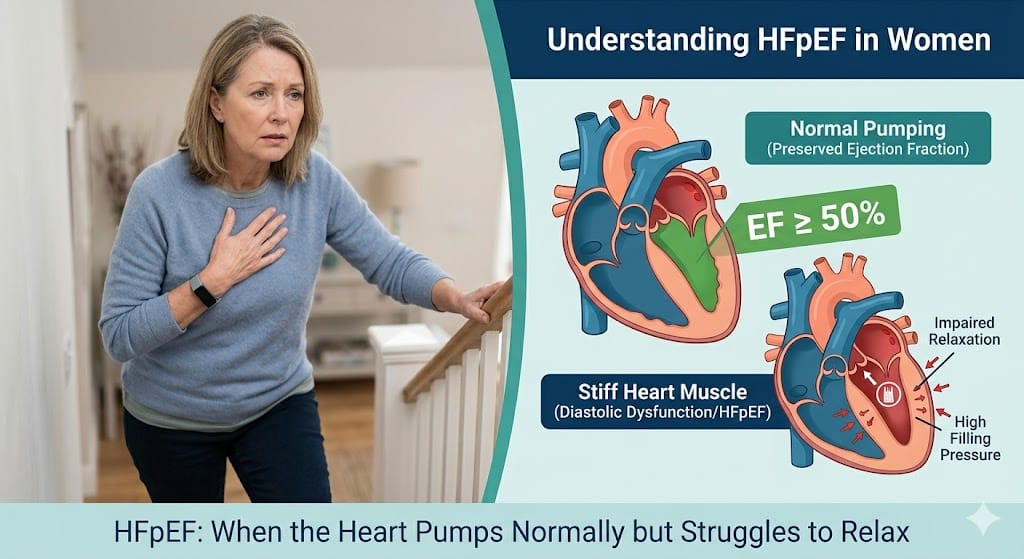
Heart failure with preserved ejection fraction (HFpEF) happens when the heart squeezes normally but fails to relax properly. A standard resting echocardiogram might show a “normal” ejection fraction. Consequently, doctors often tell patients their heart is perfectly fine. This leaves many women without crucial answers. This article explains why doctors frequently delay a diastolic heart failure diagnosis. Furthermore, you will learn exactly what diagnostic tests actually matter and how to advocate for your cardiovascular health with your specialist.
What Is HFpEF (Heart Failure with Preserved Ejection Fraction)?
HFpEF stands for heart failure with preserved ejection fraction. In this condition, your heart pumps blood out efficiently. Therefore, your systolic function appears normal. However, the heart muscle develops severe left ventricular stiffness.
This stiffness prevents the heart from relaxing fully. Consequently, the heart cannot fill with enough blood during the resting (diastolic) phase. Pressure then builds up inside the heart and backs up into the lungs. Women make up the vast majority of HFpEF patients. Changes in hormones during menopause, combined with naturally smaller heart chambers, make women highly susceptible to this stiffening process.
Why HFpEF Is Often Missed in Women
Cardiovascular diagnosis historically centers on male symptom patterns and weakened heart pumping. Therefore, doctors frequently misunderstand female presentations. Many women hear they are just anxious, stressed, or out of shape.
Furthermore, standard resting echocardiograms often miss the problem entirely. At rest, a stiff heart might cope adequately with normal blood volume. Symptoms usually trigger only during physical exertion when the body demands more oxygen. This gender bias in cardiovascular medicine leaves many women struggling for years before receiving an accurate diagnosis.
HFpEF Symptoms in Women Misdiagnosed as “Normal Aging”
Many women dismiss their changing bodies as natural aging. However, these seven signs indicate a deeper cardiovascular issue.
Unexplained Exercise Intolerance: You suddenly cannot climb stairs you easily navigated last year. This exercise intolerance HFpEF hallmark happens because the stiff heart cannot increase output during activity.
Breathlessness on Minimal Exertion: The shortness of breath on exertion women experience often gets wrongly blamed on asthma. Instead, it signals fluid backing up into the lungs.
Rapid Fatigue During Daily Tasks: This unexplained cardiovascular fatigue feels profoundly different from a poor night’s sleep. Your body literally lacks sufficient oxygenated blood flow for routine chores.
Swelling in Legs or Abdomen: Fluid retention (edema) pools in your lower extremities or stomach. Consequently, you might notice sudden, unexplained weight fluctuations.
Heart Rate Spikes with Mild Activity: Your heart attempts to compensate for poor filling capacity by beating much faster. This compensation causes uncomfortable palpitations.
Night-time Shortness of Breath: Waking up gasping for air (paroxysmal nocturnal dyspnea) occurs frequently. Lying flat pushes pooled fluid from your legs back into your lungs.
Brain Fog or Reduced Stamina: Poor forward blood flow reduces optimal oxygen delivery to the brain. Thus, patients experience cognitive heaviness and severe stamina drops.
Key Diagnostic Tests for HFpEF (What Doctors Look For)
According to the 2025 ACC/AHA Heart Failure Guidelines, diagnosing HFpEF requires specific, targeted evidence beyond standard tests.
BNP Levels in Heart Failure Diagnosis
Brain natriuretic peptide (BNP) and NT-proBNP are proteins released when heart pressures rise dangerously. Checking these BNP levels heart failure protocols mandate provides critical clues. However, HFpEF symptoms in women misdiagnosed often stem from borderline BNP blood results. Obesity naturally lowers BNP levels. Therefore, a “normal” lab result might actually hide active HFpEF in a heavier patient.
Echocardiogram HFpEF Criteria
A basic resting echo is simply not enough. Cardiologists must evaluate specific echocardiogram HFpEF criteria. First, they verify a preserved ejection fraction (EF ≥50%). Crucially, they must also measure left atrial enlargement and specific diastolic dysfunction markers. The E/e’ ratio specifically evaluates cardiac filling pressures. If your doctor only checks your EF, they miss the complete picture.
Exercise or Stress Testing in HFpEF
When resting tests look normal but symptoms persist, cardiologists must utilize dynamic stress testing. Exercise stress echocardiography reveals exactly how the heart behaves under workload. It clearly detects filling pressure rises during physical exertion. Sometimes, doctors require invasive hemodynamic testing via a right heart catheterization to confirm the diagnosis definitively.
HFpEF Diagnostic Checklist (Patient-Friendly)
Bring this practical checklist to your next cardiology appointment to guide your evaluation.
| Evaluation Area | Specific Tests & Indicators to Request |
| Symptoms | Documented breathlessness, fatigue, and edema |
| Blood Work | BNP or NT-proBNP (request adjustment for BMI) |
| Resting Echo | LVEF ≥50%, E/e’ ratio, left atrial volume index |
| Stress Testing | Exercise echocardiogram for active filling pressures |
| ECG Clues | Signs of atrial fibrillation or left ventricular hypertrophy |
| Risk Factors | History of hypertension, obesity, diabetes, or menopause |
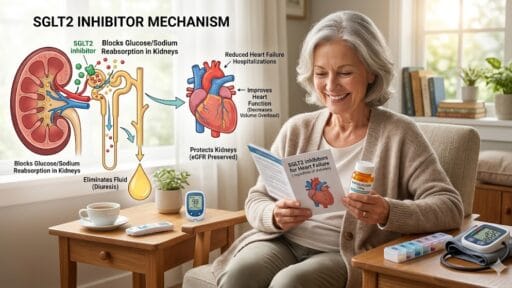
Preserved Ejection Fraction Treatment 2025 Overview
The preserved ejection fraction treatment 2025 landscape offers unprecedented hope. Current ACC/AHA guidelines heavily prioritize SGLT2 inhibitors (such as empagliflozin or dapagliflozin). These specific medications significantly reduce heart failure hospitalizations and improve survival.
Treatment also requires strict blood pressure control and targeted diuretics to manage fluid congestion. Furthermore, supervised cardiac exercise training drastically improves daily stamina. Doctors must also aggressively manage your underlying comorbidities to stabilize heart function effectively.
Risk Factors for HFpEF in Women
Several key physiological factors compound a woman’s HFpEF risk over time:
Hypertension: Long-standing high blood pressure forces the heart muscle to thicken and eventually stiffen.
Obesity: Excess weight actively increases systemic inflammation and alters internal heart structure.
Diabetes: High blood sugar damages delicate blood vessels and stiffens cardiac tissues.
Post-Menopausal Status: The sudden loss of estrogen accelerates arterial stiffening and adverse cardiac remodeling.
Coronary Microvascular Dysfunction HFpEF: Small blood vessel disease in the heart restricts oxygen delivery. This restriction directly impairs heart relaxation.
When to Seek a Cardiologist Evaluation
Do not ignore persistent, life-altering symptoms. Seek specialized cardiovascular care if you notice:
Persistent, unexplained breathlessness during basic routine activities.
Normal primary care tests, but steadily worsening physical symptoms.
A drastic, sudden reduction in your daily activity tolerance.
HFpEF in Women: Why Early Diagnosis Matters
Early detection fundamentally changes long-term patient outcomes. Treating HFpEF quickly prevents irreversible structural heart damage. Early intervention dramatically improves your daily quality of life and physical stamina. Furthermore, prompt medical management heavily reduces the risk of emergency hospitalizations. Patients simply respond much better to medical therapies when treatment begins before severe, chronic fluid overload occurs.
Frequently Asked Questions
Can HFpEF be missed on an echocardiogram? Yes. A resting echo might appear completely normal. Cardiac stiffness often causes high pressures only during physical exertion.
What is BNP in heart failure? BNP is a specialized blood marker indicating heart stress. Elevated levels suggest heart failure, though obesity can artificially lower these exact numbers.
Why do women get HFpEF more? Women naturally have smaller, stiffer hearts. Menopause-related estrogen loss and microvascular disease further increase their lifetime HFpEF risk.
Can HFpEF be reversed? HFpEF cannot be completely cured. However, modern medications like SGLT2 inhibitors and lifestyle changes can successfully halt progression and relieve symptoms.
Is HFpEF dangerous? Yes. Untreated HFpEF leads to severe fluid buildup, organ damage, and high hospitalization rates. It carries mortality risks similar to systolic heart failure.
What is normal EF but heart failure? This means your ejection fraction is 50% or higher. However, the heart muscle remains too stiff to fill properly with oxygenated blood.
What is the best treatment for HFpEF 2025? Current cardiology guidelines strongly recommend SGLT2 inhibitors. Doctors combine these with diuretics, strict blood pressure management, and supervised exercise therapy.
How is HFpEF diagnosed definitively? Diagnosis requires clinical symptoms, elevated BNP, structural echo changes, and often an exercise stress test to measure active pressures.
Is shortness of breath the only sign of HFpEF? No. Unexplained fatigue, heart palpitations, brain fog, and sudden weight gain from fluid retention are equally critical warning signs.
Should I see a general cardiologist or a heart failure specialist? If you have persistent symptoms but a “normal” echo, seek a dedicated heart failure specialist. They possess advanced training in complex diastolic dysfunction.
Conclusion
Navigating a complex cardiovascular diagnosis requires immense persistence and medical advocacy. Unfortunately, HFpEF symptoms in women misdiagnosed as normal aging or anxiety remain an alarming clinical reality. When your standard medical tests return normal, yet you can barely climb your home’s stairs, you must keep pushing for deeper answers.
Proper diastolic heart failure diagnosis requires comprehensive evaluation. This includes BMI-adjusted BNP levels, specialized echocardiography, and dynamic exercise stress testing. Do not accept simple “deconditioning” as a final answer if your body tells you something is profoundly wrong. Print the diagnostic checklist provided above and schedule a targeted consultation with a heart failure specialist. You deserve diagnostic clarity, clinical validation, and an evidence-based treatment plan to safely reclaim your quality of life.
Disclaimer: This article is for educational purposes only and does not replace professional cardiology evaluation. Always consult a qualified healthcare provider for medical advice, diagnosis, and treatment.